Hunger And Undernutrition
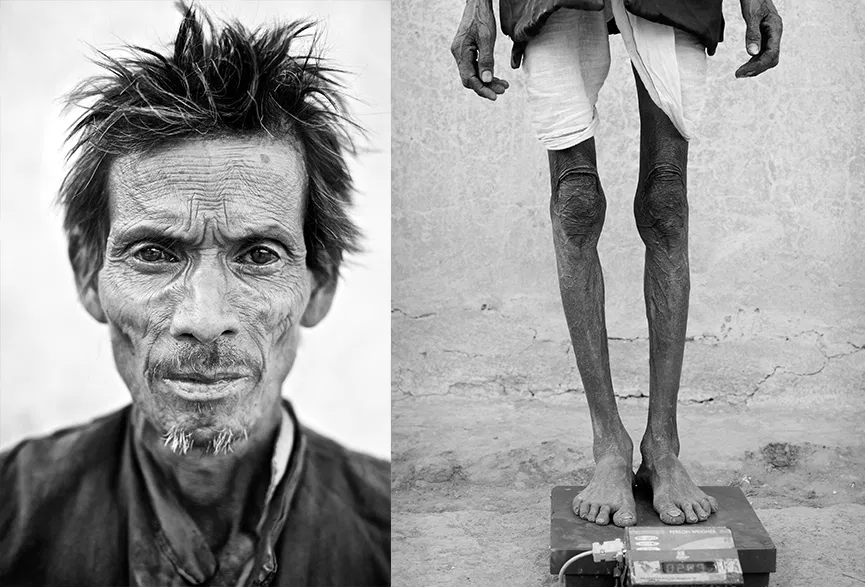
Photo by Tom Pietrasik
Or do we call it malnutrition? Or do we call it N-AIDS, the leading cause of acquired immune dysfunction?
A 2002 study in Bilaspur found that 41% of men and 43% of women had a BMI (body mass index) of less than 18.5. People with a BMI under this threshold are considered to be underweight.
The consequences of low BMI include poor work capacity, which leads to lower income, which in turn leads to less food to eat and a lower BMI. Individuals with low BMI also fall ill more frequently, and mothers with low BMIs have smaller babies.
Almost 65% of our children below the age of 5 years are undernourished. Most of the mental development occurs in early childhood, and most malnutrition sets in by the age of 2 to 3 years. This affects a child’s learning ability in school, and thus the consequences of early undernutrition are worsened.
Why are we Hungry/Undernourished?

Rice left unprotected to rot in the rain and be eaten by vermin
While India’s population and its need for food is increasing, there is currently enough food to go around. The problem is with the distribution system and accessibility.
Instead of being consumed locally, rice, the staple crop of India, has become part of an inefficient national distribution network. It is often left unprotected from the elements and animals. Prices are increasing, and rural areas do not have the economic power to harness the market forces that would pull adequate food in their direction.
Farmers who do produce rice for their own consumption are often small farmers who are at the mercy of the increasingly irregular monsoon. They also are often subject to substantial debts incurred at high interest for the purchase of seeds and fertilisers.
Illness can precipitate the situation, with both direct and secondary effects. Money that once went to food is often diverted to health care, and farm productivity and/or wages earned may be missed due to illness.
Food purchasing in Chhattisgarh

This sign indicates that the family in this house is to recieve 35 kg of rice a month at 2 rps/kg
The current policy of food grain subsidy in India, distributed through the Public Distribution System (PDS), is insufficient to provide food security to the poor. While the Chhattisgarh Government has recently started a populist programme of providing 35 kg subsidised rice (at Rs 1 or 2 per kg) per month to BPL families, this does not last a family of 5 more than 15 days. Thus, even the officially poor have to procure food grains from the open market, where prices have been spiraling upward. This sign indicates that the family in this house is to receive 35 kg of rice a month at 2 rps/kg[/caption] (Current minimum price of rice in the area is Rs. 12 per kg). In a predominantly cereal based diet, anything less than 70 kg of food grain per month per family of 4 or 5 is insufficient for maintaining good health. Although Chhattisgarh has a long way to go in securing adequate food for its people, unfortunately most other states in India do not even offer the partial support that Chhattisgarh provides.
Not only is the persistence of widespread undernourishment in India -more than in all other regions in the world – quite extraordinary, so is the silence with which it is tolerated, not to mention the smugness with which it is sometimes dismissed.
-Amartya Sen
What is particularly alarming is the recent withdrawal of any kind of subsidy on food grains to those not officially poor. In Chhattisgarh, a recent official announcement makes all families without a BPL card ineligible for any subsidised rations. This means that even the rice that was provided at Rs. 2/- per kg is no longer available, which means families are forced to buy rice at the prevailing market rates. The consequence of this on the health of people is likely to be grave.
At a family level, weights and heights are the most robust indicators for poverty status and are likely to be better than the often fallacious poverty line assessment. With such high rates of undernutrition, malnourishment is not limited to BPL families, and many more individuals deserve subsidised food rations.
What we are doing
JSS is addressing the issue of undernutrition through its crèche program and through supporting agricultural initiatives such as the system of rice intensification (SRI).
The social protection in terms of food availability that we propose is:
- 5-70 kilos food grain per family, 3 kilos of daal, and 1 kilo oilseeds or oil per month
- Weight or nutrition status based entitlements of food grains (not poverty line based)
- Supplementary food grain provision for illnesses of poverty as part of treatment, like TB